
Endocrinology
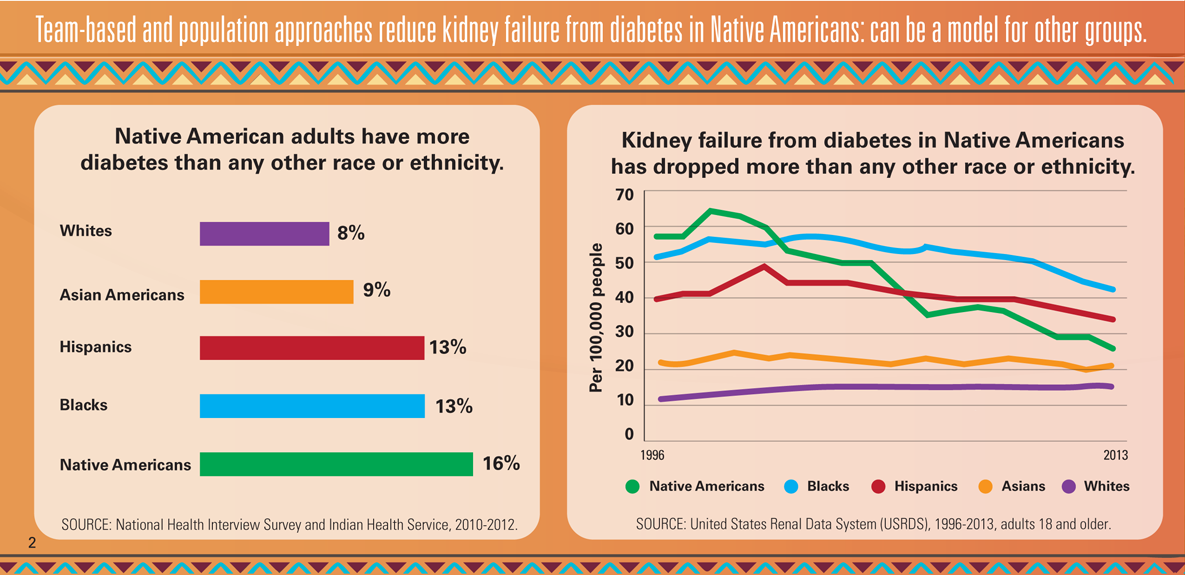
Making a difference to reduce kidney failure from Diabetes in Native Americans Team-based and population approaches can be a model for other groups Recent health surveys from the Indian Health Service show Native American adults have more diabetes than any other race or ethnicity, (Source: IHS 2010-2012). In response to the diabetes epidemic among American Indians and Alaska Natives, Congress established the SDPI grant programs in 1997. This $150 million annual grant program, coordinated by IHS Division of Diabetes with guidance from the Tribal Leaders Diabetes Committee, provides funds for diabetes treatment and prevention to IHS, Tribal, and Urban Indian health programs across the United States. This intervention has been attributed to a reduction of Kidney failure from diabetes in Native Americans, having dropped more than any other race or ethnicity. Comparing kidney failure from diabetes in Native Americans to other groups from 1996 to 2013, in 1996 Native Americans had more kidney failure than blacks, Hispanics, Asians and whites. By 2013 however, Native Americans were third in kidney failure from diabetes despite having the most diabetes. Per 100,000 people: General population (1996) (2013) (% change) American Indians/Alaska Natives (57.3) (26.5) (-54) Asians (23.1) (22.2) (-4) Blacks (52.2) (42.7) (-18) Whites (12.1) (15.5) (+28) Hispanics (40.1) (34.2) (-15) Source: United States Renal Data System (USRDS), 1996-2013, adults 18 and older. The 2014 report to Congress from Indian Health Service's Special Diabetes Program for Indians (SDPI) demonstrated tremendous improvements to key attributes in both Diabetes prevention and treatments. Current efforts such as the IHS Diabetes in Indian Country Conference are continuing to make improvements, such as the with the 2019 conference held in Oklahoma City which provided continuing education opportunities and collaboration on issues related to improving outcomes for people with diabetes and those at risk for developing diabetes. 132 onsite sessions were conducted to provide education to 1,228 attendees from 33 states. Infographics such as "A Model for Diabetes Care" depicting the story of one particular fictitious patient (Joe) includes text boxes with information about what Health Care Systems can do to reach out to entire communities Team-Based Patient Care and Population Management strategies. These points can be used in all populations effectively and have been made available for all Public Health providers to use in their local communities. Public health and population management include:
2. Care manager calls Joe because of missed doctor appointments. 3. Joe has no sick leave at work or transportation to make it to appointments or pick up his medicine. He also has trouble getting healthy food. 4. During a home visit, nurse brings Joe his medicine, checks his blood pressure, and draws blood for lab tests. 5. Nurse connects Joe to community food and transportation resources. She schedules a clinic visit for his next day off. 6. At the clinic, Joe’s doctor adjusts his medicine. Joe meets with a nutritionist and diabetes educator. 7. Pharmacist helps make sure Joe gets his medicine on time and is taking it correctly. 8. Over time, Joe’s blood pressure and blood sugar are controlled and his kidney function remains okay. The diabetes care team helps patients avoid kidney failure by:
Source: CDC |
|
Healthcare professionals receiving our publications are invited to contact us about ideas for future editions and editorial submissions by emailing fhmeditorial@capitalpublishing.com or calling 813-286-8444
© 2024 Capital Publishing Inc - All Rights Reserved